
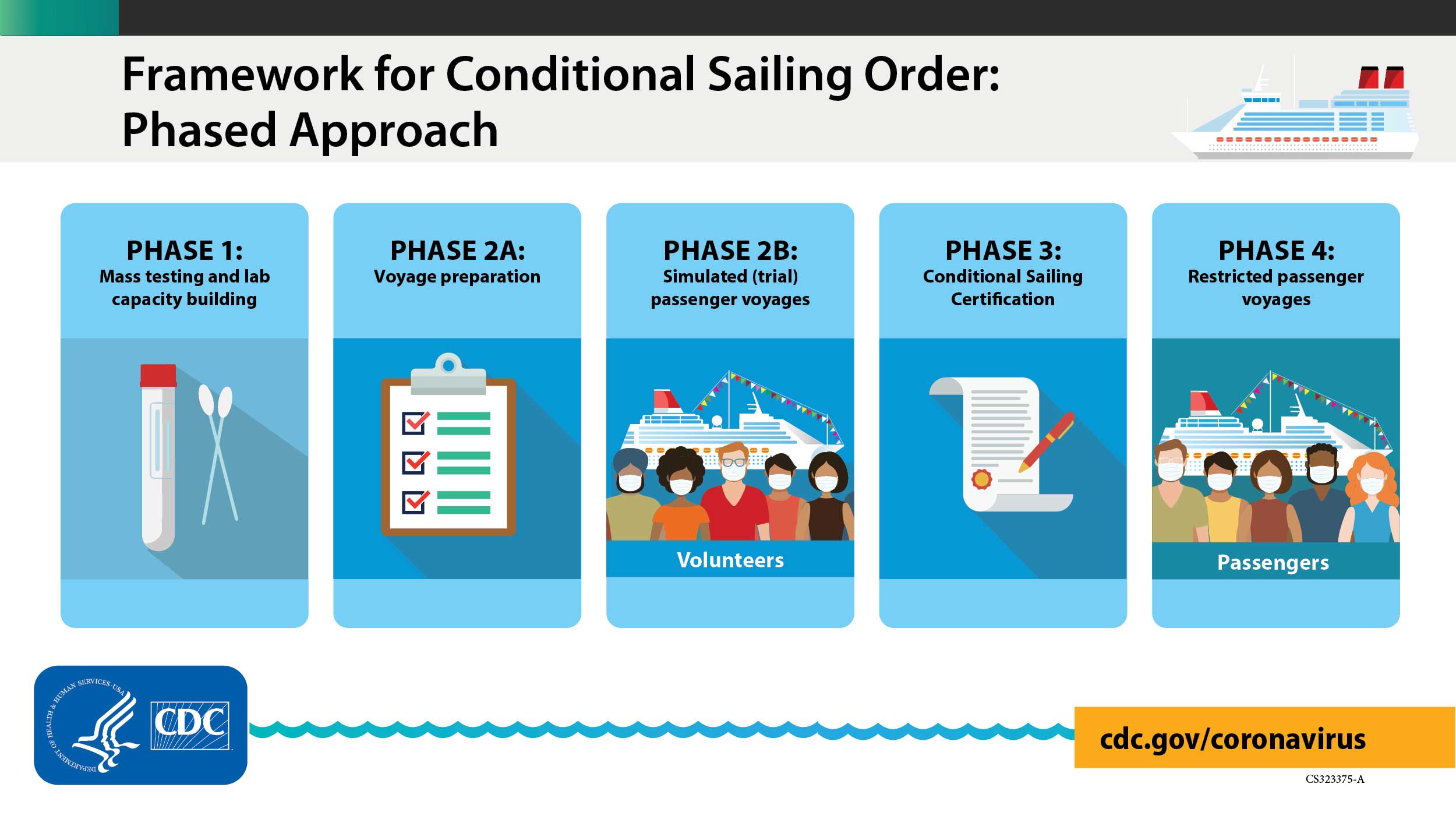
On April 2, 2021, the CDC released a new phase, Phase 2A, of the Framework for Conditional Sailing Order, which was issued over 5 months ago, for cruise ships operating or seeking to operate in U.S. waters. CDC published technical instructions for cruise ship operators and for local health authorities outlining this phase of the Conditional Sailing Order. Today’s announcement comes a week after the Florida Governor held a roundtable with cruise industry leaders at Port Canaveral and CLIA’s call to action to elected officials to push for the CDC to work with the cruise industry on a safe return to cruising.
The details released by the CDC (archived) are as follows:
Technical Instructions for a Cruise Ship Operator’s Agreement with Port and Local Health Authorities under CDC’s Framework for Conditional Sailing Order
Audience
This document is intended to assist cruise ship operators in documenting the approval of U.S. port and local health authorities as a condition of receiving or retaining controlled free pratique to conduct one or more simulated voyages or restricted passenger voyages under a COVID-19 Conditional Sailing Certificate. This includes documenting the approval of U.S. port and local health authorities in developing medical care, housing, and port components (including a vaccination component) of an agreement as per the terms of CDC’s Framework for Conditional Sailing Order.
Purpose
This document provides instructions for Phase 2A of CDC’s Framework for Conditional Sailing Order for cruise ship operations in U.S. waters to ensure health and safety protections for travelers (crew and future passengers) and port personnel prior to resuming passenger operations in a way that mitigates the risk of spreading COVID-19.
As required by the terms of CDC’s Framework for Conditional Sailing Order, a cruise ship operator must document the approval of all U.S. port and local health authorities where the ship intends to dock or make port during one or more simulated voyages or restricted passenger voyages as a condition of receiving or retaining controlled free pratique for conducting one or more simulated voyages or receiving and retaining a COVID-19 Conditional Sailing Certificate.
These instructions are not intended as, and do not constitute, a comprehensive statement regarding a cruise ship operator’s duties and obligations under CDC’s Framework for Conditional Sailing Order. These instructions reflect CDC’s reasoned judgement based on the best available current science regarding the subject areas covered in the document. Cruise ship operators, U.S. port authorities, and local public health authorities should carefully consider and incorporate these instructions in developing their own health and safety protocols.
In deliberating with cruise ship operators, U.S. port authorities and local health authorities consistent with their own jurisdiction’s legal authorities, needs, and local considerations may impose additional requirements that reflect a higher level of public health protection than in this document and do not otherwise conflict with CDC’s exercise of federal authority. Additionally, U.S. port authorities and local health authorities should take into consideration CDC’s Interim Public Health Recommendations for Fully Vaccinated People. For purposes of these instructions, CDC considers cruise ships to constitute a residential congregate setting.
CDC may update these instructions for cruise ship operators for the additional phases (Phases 2B through 4) of resuming cruise ship passenger operations. These additional phases will be further described in future technical instructions and/or orders. CDC will notify cruise lines when these instructions are updated.
General Components of a Cruise Ship Operator’s Agreement with Port and Local Health Authorities
- For the purpose of these technical instructions only, “local health authorities” refers to all health departments responsible for implementing state, territorial, and local laws relating to public health (e.g., city, county, territorial, and/or state health departments) and exercising jurisdiction over the U.S. port where the cruise ship operator intends to conduct one or more simulated voyages and commence restricted passenger operations.
- For the purpose of these technical instructions only, “U.S. port authorities” refers to officials responsible for exercising oversight and control over the U.S. port where the cruise ship operator intends to conduct one or more simulated voyages and commence restricted passenger operations.
A cruise ship operator must document the approval of all U.S. port and local health authorities where the ship intends to dock or make port during one or more simulated voyages or restricted passenger voyages as a condition of receiving or retaining controlled free pratique for conducting one or more simulated voyages or obtaining and retaining a COVID-19 Conditional Sailing Certificate. Such written approval must include the following general terms and conditions:
- The parties to the agreement are the cruise ship operator, U.S. port authority where the cruise ship operator intends to conduct one or more simulated voyages and commence restricted passenger operations, and all health departments exercising jurisdiction over the port.
- The cruise ship operator must seek CDC approval before adding any additional parties or substituting parties to the agreement.
- Parties to the agreement may not assign or transfer responsibilities without prior CDC approval.
- The agreement must include a port operations component (including a vaccination component), a medical care plan component, and a housing component meeting the requirements of these technical instructions. These components should be attached as annexes to the agreement and will be deemed to constitute a part of the agreement.
- There should be one agreement between the cruise ship operator and all relevant U.S. port and local health authorities per port. If it is expected that more than one cruise ship operator will be operating ships out of the U.S. port, then the relevant U.S. port and local health authorities should enter into separate agreements with each cruise ship operator. CDC does not seek to limit the number of separate agreements that U.S. port and local health authorities may enter into with cruise ship operators but defers to these authorities.
- Deliberations should be conducted jointly between the cruise ship operator and all relevant U.S. port and local health authorities.
- Cruise ship operators should not enter into separate agreements with U.S. port and local health authorities. However, the agreement may be executed in any number of separate counterparts, all of which when taken together will constitute one and the same agreement.
- The agreement is intended solely for the benefit of the parties involved. The agreement should not be viewed as conveying any rights or benefits on any third parties not a party to the agreement.
- The agreement must specifically list the names of the cruise ship operator’s ships covered by the terms of the agreement.
- The agreement must include the total number of ships (including maximum number of travelers (passengers and crew)) permitted to operate, make port, embark, or disembark. The parties to the agreement should jointly consider the number of ships (including maximum number of travelers (passengers and crew)) that can safely operate, make port, embark, or disembark at any one time without exceeding the ability of local public health, port authority, hospital, and other emergency response personnel to respond to an onboard outbreak of COVID-19. The agreement should briefly explain the factors relied upon by all parties in determining these numbers, including the potential for COVID-19 variants, which could undermine vaccine efficacy.
- The agreement must be specific regarding the following:
- number of ships that will be permitted to make port, embark, and disembark,
- hours of the day, and days of the week, and during which these activities will occur, and
- maximum number of travelers permitted during those hours and on those days.
- If the port authority intends to allow more than one cruise ship operator to operate at its port facilities, then the port authority and local public health authorities should jointly consider the numbers of ships and maximum number of travelers (passengers and crew) that can safely operate, make port, embark, or disembark at any one time. Specifically, the parties should consider whether allowing multiple cruise ships to operate at any one time would potentially overwhelm necessary medical supplies or the ability of local public health, port authorities, hospital, and other emergency response personnel to respond to an onboard outbreak of COVID-19, particularly if the jurisdiction experiences an unanticipated simultaneous surge of cases.
- Parties to the agreement should maintain the right to modify, amend, or rescind the agreement. The cruise ship operator must immediately notify the CDC if an agreement is modified, amended, or rescinded. The parties should also jointly consider the need to temporarily suspend or rescind an agreement if resources in the local community (e.g., local public health, port authority, hospital, or emergency response personnel) become insufficient to adequately respond to an onboard outbreak of COVID-19 on a cruise ship.
- U.S. port authorities and local health authorities should monitor and enforce compliance with the agreement. However, in the event that the U.S. port and/or local health authorities choose to temporarily suspend or rescind the agreement, such suspension or rescission cannot deny a cruise ships’ ability to make port as approved by the CDC if on a voyage.
- Local health authorities should determine their requirements for reporting of cases identified during a voyage, including thresholds for reporting, timelines, reporting mechanisms, and points of contact. Such reporting requirements, if any, should be incorporated into the agreement and may be in addition to but not replace CDC-mandated reporting by cruise ship operators.
- The agreement must be signed and executed, and a copy (including all attachments, exhibits, and annexes) provided to CDC, prior to CDC’s approving a cruise ship operator’s request to embark non-essential crew.
- A copy of the signed and executed agreement (including all attachments, exhibits, and annexes) must also be provided to CDC as part of a cruise ship operator’s application to conduct one or more simulated voyages. CDC will provide additional information about simulated voyages in future technical instructions and orders.
- The signatories to the agreement must include the following:
- The cruise ship operator’s responsible officials, meaning the Chief Executive Officer (or equivalent) of the operating cruise company and all parent companies, the Chief Compliance Officer (or equivalent) of the operating cruise company and all parent companies, and the highest-ranking Medical Officer of the operating cruise company and all parent companies.
- The highest-ranking officials for all relevant local public health authorities, except that such officials may delegate at their own discretion.
- The U.S. port authority’s highest-ranking official. This individual will typically be designated as the Port Director/Chief Executive Officer.
- A checklist for the agreements listed below will be available by email upon request. U.S. port authorities, local health authorities, and cruise ship operators may contact CDC at eocevent349@cdc.gov for these templates. The request should include “Agreements Checklist” in the subject line.
Vaccination Components of a Cruise Ship Operator’s Agreement with Port and Local Health Authorities
CDC recommends that all eligible port personnel and travelers (passengers and crew) get a COVID-19 vaccine when one is available to them. Parties to an agreement between a cruise ship operator and U.S. port and local health authorities should ensure that the agreement additionally incorporates the following components relating to vaccination of port personnel, crew, and future passengers:
- A plan and timeline for vaccination of cruise ship crew prior to resuming passenger operations. Due to the international representation of cruise travelers, cruise operators must use either U.S. Food and Drug Administration (FDA)-authorized vaccines or a vaccine product that has received emergency use listing from the World Health Organization (WHO).
- Presentation of proposals regarding how the cruise ship operator intends to incorporate vaccination strategies to maximally protect passengers and crew from introduction, amplification, and spread of COVID-19 in the maritime environment and land-based communities.
- Designation of a cruise ship operator vaccine coordinator to oversee implementation and maintenance.
- Implementation of processes for vaccinating crew currently onboard as well as newly embarking crew. If any adverse events occur, a cruise ship clinician should report them to the Vaccine Adverse Events Reporting Systemexternal icon (VAERS) for FDA-authorized vaccines and through appropriate reporting mechanisms for vaccines approved for use by other countries. See VAERS Frequently Asked Questionsexternal icon for additional information.
- Education of port personnel and travelers about the importance of getting COVID-19 vaccine.
- Implementation of processes for vaccinating port personnel who are expected to interact with travelers.
- Port authorities and cruise ship operators should consider hosting vaccination clinics for port personnel who are expected to interact with travelers. Port employers should encourage employees who are expected to interact with travelers to get a COVID-19 vaccine when one is available to them and give employees information about how to get vaccinated locally.
Fully vaccinated port personnel and travelers are still subject to all of the requirements of CDC’s Order requiring wearing of masks on conveyances entering, traveling within or leaving the United States, and in U.S. transportation hubs (see maritime-specific Frequently Asked Questions).
Additional Port Components of a Cruise Ship Operator’s Agreement with Port and Local Health Authorities
Parties to an agreement between a cruise ship operator and U.S. port and local health authorities should ensure that the agreement additionally incorporates the following components relating to maintaining the health and safety of port personnel:
- The agreement must specify embarkation procedures that the cruise ship operator intends to use during simulated voyages and restricted passenger voyages. These embarkation procedures must be designed insofar as possible to minimize contact between travelers and port personnel. CDC may request that the parties modify or amend the agreement to reflect changes to embarkation procedures based on “lessons learned” from the cruise ship operator’s simulated voyage(s) as described in the after-action report for each voyage.
- The agreement must specify procedures for day-of-embarkation screening for signs and symptoms of COVID-19 and laboratory testing of travelers, including testing locations and management of individuals who test positive and their close contacts.
- The agreement must include emergency response plans in the event of a “worst case” scenario of multiple ships experiencing simultaneous outbreaks of COVID-19. If the port authority intends to allow more than one cruise ship operator to operate at its port facilities, then the port authority and local public health authorities should jointly consider emergency response plans involving a “worst case” scenario of multiple ships from multiple cruise ship operators experiencing simultaneous outbreaks of COVID-19.
- The agreement must include clear protocols for contacting emergency medical services while at port for exigent circumstances not covered by the hospital component of the agreement (e.g., a medical emergency not related to COVID-19, such as a heart attack).
- The agreement must include clear protocols that avoid medical evacuations at sea to the greatest extent possible for both COVID-19 and non-COVID-19 related medical reasons. Protocols must rely on commercial resources (e.g., ship tender, chartered standby vessel, chartered airlift) for unavoidable medical evacuation at sea and be designed to minimize the burden to the greatest extent possible on Federal, State, and Local government resources, including U.S. Coast Guard resources. All medical evacuations at sea must be coordinated with the U.S. Coast Guard.
- The agreement must specify disembarkation procedures that will be implemented in the event of an outbreak of COVID-19, and that the cruise ship operator intends to use during simulated voyages and restricted passenger voyages. CDC may request that the parties modify or amend the agreement to reflect changes to disembarkation procedures based on “lessons learned” from the cruise ship operator’s simulated voyage(s) as described in the after-action report for each voyage.
- The agreement must specify procedures:
- to avoid congregating of embarking and disembarking travelers,
- to ensure disembarking and embarking passengers do not occupy the same enclosed or semi-enclosed areas (e.g., gangways, terminal waiting spaces, check-in areas) within the same 12-hour period, and
- to ensure disembarking and embarking travelers from different ships do not occupy the same enclosed or semi-enclosed areas (e.g., gangways, terminal waiting spaces, check-in areas) within the same 12-hour period.
- The agreement must include procedures for informing port personnel who are expected to interact with travelers (passengers and/or crew) of the risks of COVID-19 and how to prevent exposure.
- It is recommended that the parties to the agreement consider incorporating specific procedures for routine testing and symptom monitoring of port personnel who are expected to interact with travelers (passengers and/or crew). Additionally, employers should encourage employees to get a COVID-19 vaccine when one is available to them and give employees information about how to get vaccinated locally. This includes but is not limited to the following personnel:
- Port agents/greeters
- Security personnel
- Transportation staff
- Baggage handlers
- Check-in staff
- Cleaners/janitorial staff
- Longshoremen
- Maritime pilots
- Delivery drivers
- The agreement must include routine and outbreak-level cleaning procedures for areas where travelers are reasonably expected to gather or otherwise make use of, including terminals and restrooms. The agreement must also include routine and outbreak-level cleaning procedures for transportation vehicles under a cruise ship operator’s control (e.g., buses, shuttle vans). For more information about cleaning and disinfection, please refer to CDC’s Detailed Disinfecting Guidance for Facilities and Cleaning and Disinfection for Non-emergency Transport Vehicles.
- It is recommended that commercial transportation companies/drivers be provided with information on cleaning procedures (taxi, ride share services, parking lot shuttle vans). For this industry, please refer to CDC’s COVID-19 webpage for Specific Industries.
Medical Care Components of a Cruise Ship Operator’s Agreement with Port and Local Health Authorities
As required by the terms of CDC’s Framework for Conditional Sailing Order, a cruise ship operator’s agreement with all U.S. port and local health authorities where the ship intends to dock or make port during one or more simulated voyages or restricted passenger voyages must incorporate medical care agreements between the cruise ship operator and health care entities, addressing evacuation and medical transport to onshore hospitals for passengers or crew in need of care, in accordance with CDC technical instructions and orders.
Parties to an agreement between a cruise ship operator and U.S. port and local health authorities should ensure that the medical care component of the agreement includes the following:
- The cruise ship operator must document that it has made contractual arrangements to provide for the emergency medical transportation of critically ill persons with suspected or confirmed COVID-19 from the ship to a shoreside medical facility in such as manner as to minimize potential for exposure.
- The cruise ship operator must document that it has made contractual arrangements with a shoreside medical facility or healthcare system or multiple shoreside medical facilities or healthcare systems with redundant capacities to ensure that travelers receive appropriate clinical evaluation, including testing, and medical care when needed.
- This requirement is to reduce the need to divert patients to other medical facilities or healthcare systems that do not have such a contractual arrangement with the cruise ship operator.
- If the cruise ship operator intends to rely on the services of a single medical facility or healthcare system, it must document that it has made contractual arrangements with a second medical facility or healthcare system if its primary medical facility or healthcare system is unable to accept additional patients or provide the necessary level of care.
- The cruise ship operator must document that its contractual shoreside medical facilities or healthcare systems either singularly or collectively have enough medical capacity in the judgement of the local health authorities to care for travelers if an unanticipated outbreak of COVID-19 occurs on board its ships. The cruise ship operator’s contractual shoreside medical facilities or healthcare systems should have enough bed capacity for both potential intensive care and non-intensive care needs, as well as enough capacity to isolate patients with COVID-19.
- The parties to the agreement must jointly consider the potential medical care needs of travelers including the capacity of local public health, port authority, hospital, and other emergency response personnel to respond to an onboard outbreak of COVID-19. The agreement must briefly explain the factors relied upon by all parties in determining the capacity of the cruise ship operator’s contractual shoreside medical facilities or healthcare systems.
- The parties to the agreement must jointly evaluate the need for further contingency planning to provide medical care to travelers in the event of limited hospital beds, medical personnel, or other factors potentially limiting the capacity of the cruise ship operator’s designated shoreside medical facilities or healthcare systems. The agreement must briefly explain the outcome of these deliberations.
Housing Components of a Cruise Ship Operator’s Agreement with Port and Local Health Authorities
As required by the terms of CDC’s Framework for Conditional Sailing, a cruise ship operator’s agreement with all U.S. port and local health authorities where the ship intends to dock or make port during one or more simulated voyages or restricted passenger voyages must incorporate housing agreements between the cruise ship operator and one or more shoreside facilities for isolation and quarantine of persons with suspected or confirmed COVID-19 and close contacts, respectively, identified from the day of embarkation through disembarkation for each voyage, in accordance with CDC technical instructions and orders.
Parties to an agreement between a cruise ship operator and U.S. port and local health authorities should ensure that the housing component of the agreement incorporates the following:
- The cruise ship operator must document that it has made contractual arrangements (or has corporate-owned shoreside housing facilities) in sufficient quantities to meet the shoreside housing needs of travelers (passengers and crew) for isolation and quarantine identified from the day of embarkation through disembarkation for each voyage. In determining sufficient quantities of shoreside housing for isolation and quarantine, the parties should consider the potential for COVID-19 variants, which could undermine vaccine efficacy. The parties may consider the following options for crew who are considered close contacts but have tested negative for COVID-19:
- All crew quarantine on board the ship provided that all crew can be housed in single-occupancy cabins with private bathrooms. Essential crew may have a working quarantine (i.e., continue working with appropriate public health measures such as social distancing and face masks).
- Essential crew stay on board the ship for a working quarantine (i.e., continue working with appropriate public health measures such as social distancing and face masks) while nonessential crew quarantine shoreside.
- All crew quarantine shoreside and essential crew are replaced with a contingent of alternate personnel.
- The agreement must consider where the ship will be physically located during the isolation and quarantine period (i.e., at the pier or at anchor). The parties to the agreement must jointly consider the potential housing needs of travelers including the capacity of local public health, port authorities, hospital, and other emergency response personnel to oversee and monitor the housing needs of travelers under isolation and quarantine. The agreement must briefly explain the factors relied upon by all parties in determining the sufficiency of the cruise ship operator’s contractual or corporate-owned shoreside housing facilities.
- The cruise ship operator must document that it has made contractual arrangements (or has corporate-owned shoreside housing facilities) in sufficient quantities as determined by the local health authorities to meet the housing needs of travelers until they meet CDC criteria to discontinue isolation or for the CDC-recommended quarantine period.
- The cruise ship operator must document that it has made contractual arrangements (or has corporate-owned vehicles) in sufficient quantities to meet the transportation needs of all travelers from the ship to the shoreside housing facilities and from the shoreside housing facility to the contractual medical facilities or healthcare systems if needed with precautions in place to avoid exposure of vehicle operators.
- Shoreside housing must meet CDC guidelines for isolation or quarantine including separate bedrooms, separate bathrooms, no shared living spaces for individuals who are not part of the same household, and the ability to separate infected persons within households from those not known to be infected.
- Shoreside housing must provide separate ventilation systems for all travelers who are not part of the same household.
- The parties to the agreement must also jointly consider the following needs of travelers (passengers and crew) under quarantine and isolation and briefly explain the outcome of these deliberations in the agreement:
- Availability and frequency of testing including the logistics of specimen collection and transportation of specimens to laboratories for testing.
- Availability of mental health services, pharmacy delivery, and other essential services.
- Availability of security, including legal considerations, to prevent travelers from violating the terms of any mandatory isolation or quarantine, and a mechanism to notify public health authorities immediately in the event that a traveler attempts to violate such terms.
- A check-in process, including delivery of luggage, designed insofar as possible to minimize contact between exposed travelers and unexposed persons.
- Procedures to ensure the daily monitoring of travelers in quarantine, including points of contact for travelers to notify if symptoms develop in between symptom checks.
- Procedures to minimize contact between travelers in quarantine and/or isolation and support staff, while still ensuring the delivery of essential services:
- Food delivery
- Laundry services
- Cleaning and linen change
- Garbage pick up
- Post-quarantine cleaning and disinfection procedures
- Post-isolation and post-quarantine procedures to allow travelers to safely return to their home communities.
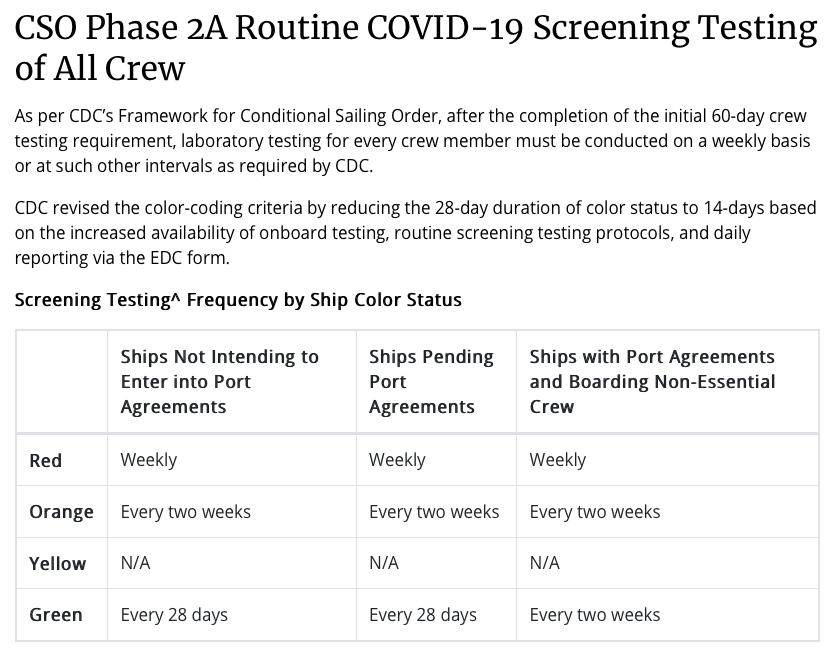
The CDC also added routine COVID-19 laboratory screening testing of all crew (archive) section, the procedures for embarking contractors overnight and visitors overnight section, and the procedures for embarking day contractors and day visitors section. As well as clarifying laboratory parameters and testing options. Updated surveillance reporting requirement to daily, revised the color-coding system, and COVID-19-like illness definition.
So the next question is…. When will Disney start ‘test sailings’?
How does a fully vaccinated person sign up for test sailings?
it is my understanding that the so called “Test Sailings” component of the “Conditional Sail Order” has been removed
I know this is good news but still not sure about my Oct cruise
Our cruise we would have had last month was canceled that we booked while on our 2019 DCL. So we rebooked for March 2022. Lets hope this gets worked out by then but we REALLY hope it gets worked out by this summer. Cruising will be the one thing we all need to get us back to normal. I wish that we all get to cruise again and soon!
Still not sure about my Panama Canal cruise in November. It sounds like they will leave in the restrictions on length of cruise. 😬
“The agreement must specify procedures:
to avoid congregating of embarking and disembarking travelers,
to ensure disembarking and embarking passengers do not occupy the same enclosed or semi-enclosed areas (e.g., gangways, terminal waiting spaces, check-in areas) within the same 12-hour period, and
to ensure disembarking and embarking travelers from different ships do not occupy the same enclosed or semi-enclosed areas (e.g., gangways, terminal waiting spaces, check-in areas) within the same 12-hour period.”
Looks like there will need to need for a new B2B process. Completely separate area, remain on board or something else.
If the masks work, why is a vaccine necessary; if the vaccine works why are the masks necessary? We all know the answers to these questions really have nothing to do with “following the science”.
The vaccines are 95% effective at preventing infection, not as effective at preventing transmission. So the mask reduces the potential for a vaccinated person for whom the immunity did not develop or the vaccinated and immune but transmissive person from spreading the virus. The whole idea of masks, distancing, hand washing, etc, is that none is perfect, but as you layer on the levels of protection you lower the potential for spread.
Mind you, just look at how some react when politely asked to wash their hands before entering MDR…
Darren, I agree. Handwashing, not going to public places when ill, covering your mouth when you cough, your nose when you sneeze—–we were all taught that by kindergarten. Feel bad for those who didn’t listen and learn or just have no common sense. Jake, thanks for the time you took to respond to what were rhetorical questions. Bon Voyage!